
Febuary blog
Please submit representations diectly
to
Professor
Leng
Royal Society of Medicine
1 Wimpole Street
London
W1G 0AE
and avoid "the enemy"-DHSC
Leng.Review@dhsc.gov.uk
Start with the premise that the NHS and Social
Care is the best UK achievement-and prioritse improving it.
Norway, Iceland, Denmark have no debt, a good NHS-they tax oil.
Change to an insurance system is humongously expensive and disruptive, will
increase the cost of living (as private dentistry has...)
GPs are the bedrock of the NHS system-prioritise increasing numbers of GPs, increasing med school places and training places over PAs-which are a drag on the system,
and fund these extra GPs properly!!!
https://www.cogora.com/cogora-general-practice-workforce-white-paper/
Cogora GP workforce crucial, important
The Great NHS Heist crucial, long but riviting
PAs in Centene GP practice frightening
Elective ringfenced funding axed
Allyson Pollock Privatisation crucial
Why Doctors & Nurses are leaving important
Reasons to leave NHSdentistry important
Pay by
-Stop overseas tax havens
-Tax oil
-Collect all taxes due.
-Tax Amazon, Google properly.
-Recover Di Do's £37 billion
There are approx 3,500 trained GPs ready to work-but the DH will not fund them: but they will fund useless PAs through ARRS
Remove tuition fees for medical school-this is a national emergency.
Remove fees for nursing-or reinstate bursaries: there is huge drop in applications.
Stop training PAs, AAs-and use the money to increase A & E staffing,
beds, admission cubicles, assess to discharge cubicles (to speed ambulance drop
offs, reduce bed blocking).
Increase number of ambulances and drivers, paramedics
Bed numbers
PFI forced smaller hospitals with fewer beds, doctors, nurses...
Uk hass 2.5 beds per 1000 people-Uk most obese, unhealthy
Germany 7.9
Austria 7.2
France 5.8
Belgium 5.6 Phil Hammond
Labour have given GPs a modest increase in funding-but NI rises swallow it all
New "Advice and Guidance fee purely to avoid hospital!!!
Upgrade NHS app for
- self referral for scans, tests-unecessary surge in workload!
-five providers(maybe miles away,
or private chop shop ISTC
-need to be simple, low-risk for
private chains
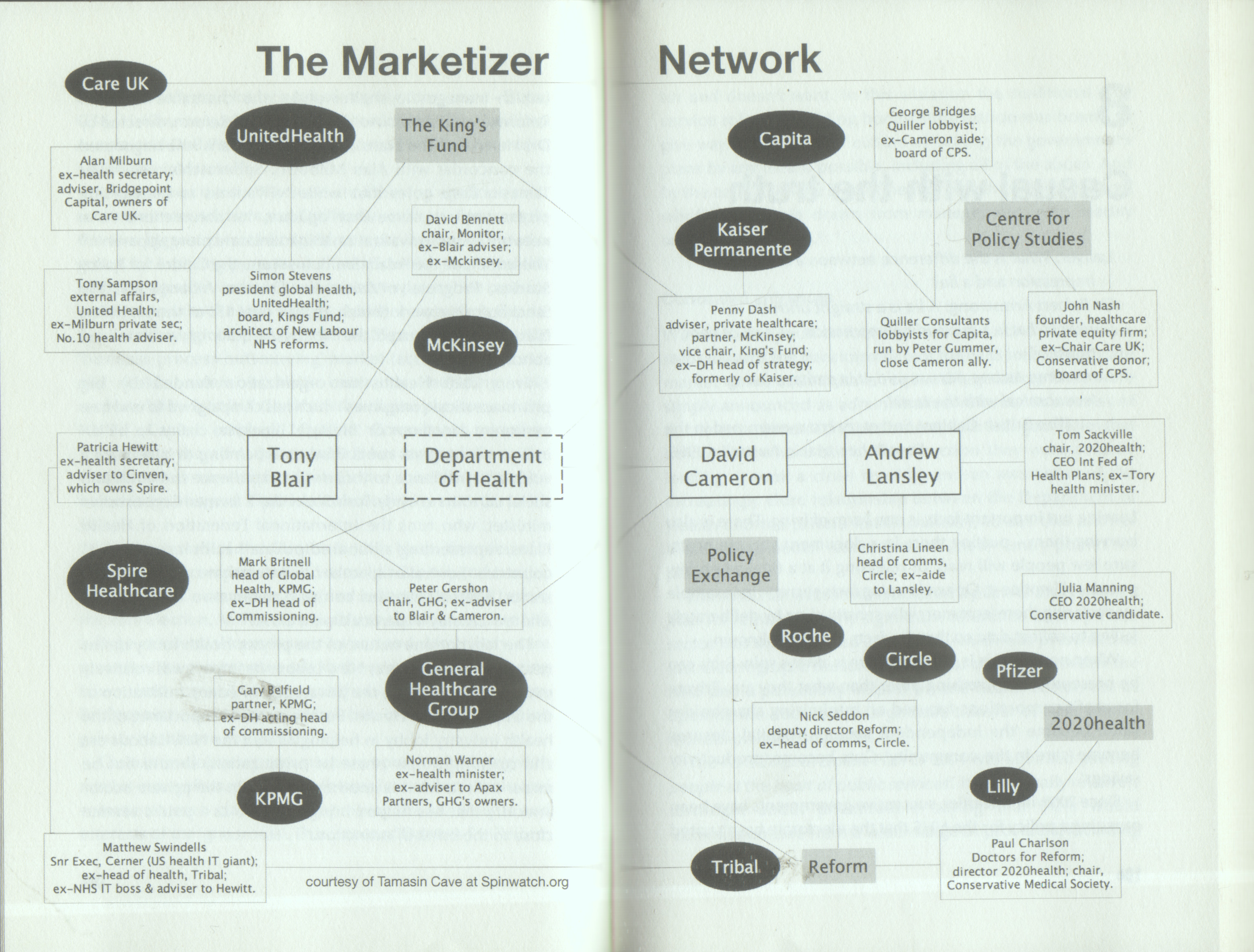
Back in 2012, dozens of lobbyists for Marketization, privatisation, outsourcing were baked into government and DHSS...
John Lister: The Lowdown
This week, the Labour government announced yet another enquiry on social care,
to an audible groan, and as we publish this article, the Guardian reveals details
of further proposals to cut the waiting times for diagnostic tests and report
a dubious response from NHS staff.
A week or so before Christmas, Labour’s Health secretary, Wes Streeting,
delivered a self-congratulatory Zoom update to Labour activists on what they
had achieved in government since winning the election in July.
He declared, “The very worst day in government is better than the best
day in opposition,” and told Labour members that ministers should be judged
by what they deliver.
But even as he spoke, stressing the level of historic underfunding and inadequate
capacity revealed by the Darzi Report and happily blaming the Tories for the
dire situation and ‘bumpy ride’ the NHS was facing this winter,
new figures emerged to show just how difficult life has become once more for
front-line staff in NHS emergency departments.
Slow progress on the fundamentals
As staff battle the ‘quad-demic’ of flu, COVID-19, RSV,
and norovirus plaguing hospitals, the lack of sufficient beds still impedes
them, as do inadequate community and primary care resources and limited social
care.
This means they struggle to discharge patients efficiently after treatment, leading to blocked beds, delays in emergency admissions, congestion in A&E, and long ambulance queues that have been making headlines again.
Worse still, there is little reason to expect this to change much by next winter— as the Labour promise for the NHS has effectively been stripped back to a long-range promise to reduce waiting lists (by March 2029).
Only modest progress has been made so far. The most recent (October) figures show that the total number of procedures patients are waiting for in England is only 230,000, lower than the peak figure of 7.77 million in September 2023. A recent HSJ report has warned that the pace of reduction of the total waiting list fell back in October:
“If the government is to deliver its pledge to restore 18-week waits by
2029, the acceleration needs to resume until the list is shrinking by one million
patient pathways per year. But in October the rate of improvement paused at
less than 200,000 a year.”
Distracted by savings targets
Part of the reason for this is financial pressures. As The Lowdown has highlighted,
ICBs are still struggling to deliver a massive £8 billion in ‘efficiency
savings’ for 2024-25. Much of the extra money from the Budget has already
been committed, and it will likely make little overall difference.
Our investigation found that NHS leaders identify common reasons for their financial difficulties: the increasing number of mental health patients with more complex issues who require admission, more patients needing ‘special’ care, a rise in serious A&E cases, and higher prescribing costs.
The extra money in Rachel Reeves’ budget has only partially reduced local
deficits. Far from building the workforce to meet the needs of the future, our
survey of ICSs revealed that workforce restrictions, such as recruitment freezes
and cuts in agency and bank staff, are the main response to the centre’s
demands for efficiency savings. These restrictions undermine safety, quality
of care, and efforts to address waiting lists.
Cash squeeze
Limits on capital spending that have increased the bill for backlog maintenance
to almost £14 billion have run alongside continued restrictions on revenue
budgets. Just before Christmas, an HSJ report echoed Lowdown analysis, noting
that all but three (39 of the 42) Integrated Care systems were falling behind
their financial plans for 2024/25, with overspending running way above forecast
levels.
The model of a universal, free-at-the-point-of-use NHS works. This ‘NHS for all’, publicly owned, provided, and accountable has frequently been ranked one of the best health care systems in the world. It is not the model that is broken, it is governments that have failed the NHS – and the population they are there to serve.
The NHS founding principles were sound, but the steady privatisation and defunding of our NHS has led to the worst crisis and worst performance in its history. We must change course before the service collapses completely.
Keep Our NHS Public
We are calling for
A PUBLICLY PROVIDED NHS: END PRIVATE INVOLVEMENT
-Ensure access to health care is based on need, free at the point of use
- Uphold the founding principles of the NHS: universal, comprehensive care
- Provide free NHS care and treatment for everyone in the UK at the time of
need
-Abolish NHS charges for migrants living in the UK
- End the myth that privatisation brings efficiency
- Commit to all NHS clinical and support services being publicly funded and
managed, and bring back outsourced services into the NHS where they belong-
End the diversion of NHS funding into private hospitals
- No more NHS disintegration and private involvement on Integrated Care Boards
-end American corporate influence with the demolition of the UK welfare state
In 1982 the Conservative Prime Minister Margaret Thatcher called a special Cabinet meeting to discuss the future demolition of the UK welfare state. With cross-party agreement, every government since Thatcher has worked towards that ultimate goal without the mandate of the British people.
In 1992 the John Major Conservative administration invited the American corporate giant UnumProvident Insurance to consult with the UK government regarding future welfare claims management, for claimants of long-term sickness and disability benefits. By 1994 the company were listed as official government advisers, and by 1999 UnumProvident Insurance were identified in a Parliamentary debate as refusing to pay income protection insurance policies to genuine claimants. Yet, this American corporate giant’s influence with UK social policy reforms helped to create the agenda for the future demolition of the welfare state, with a 2005 official corporate document quoting Unum’s Chief Medical Officer confirming that the future UK welfare reforms were ‘…to a large extent being driven by our thinking and that of our close associates ’.
At the same time as funding the ‘UnumProvident Centre for Psychosocial and Disability Research’ at Cardiff University for the first five years, the company were being identified in 2005 as ‘an outlaw company ’ by John Garamendi, the California Department of Insurance Commissioner, which was disregarded by the Blair New Labour government as the planned demolition of the UK welfare state was pursued.
In 2006 UnumProvident Insurance provided a detailed memorandum for the Work and Pensions Select Committee, which clearly listed the transformation of the long-term sickness and disability benefit known as Incapacity Benefit to the new Employment and Support Allowance (ESA). The requirement to ‘resist diagnosis ’, ‘change the name of Incapacity Benefit ’ and ‘benefits not to be given on the basis of a certain disability or illness but on capacity assessments ’ have all come to pass, as demonstrated by the use of the Work Capability Assessment (WCA), which uses all those listed suggestions to limit access to the ESA benefit for people who are too ill to work.
Historically, UnumProvident Insurance were banned in fifteen states in America and six countries worldwide until 2008. Professor John Langbein of the Yale School of Law produced an academic paper in January 2007 identifying the ‘UnumProvident Scandal ’ that exposed Unum’s practice of disability denial, and in 2008 the American Association for Justice identified Unum as the second worst insurance company in America. UnumProvident Insurance changed its name to Unum Insurance in 2007 following negative publicity and, in November 2007, BBC News reported that the British government were being advised by an American insurance company with a reputation for ‘racketeering’.
The Work Capability Assessment
Introduced in October 2008 by the New Labour government, with the former Chancellor Gordon Brown as the new Prime Minister, the Work Capability Assessment (WCA) is a dangerous and fatally flawed assessment, adopted by the Department for Work and Pensions (DWP) using the notorious Waddell and Aylward biopsychosocial (BPS) model, which would eventually be used for assessments linked to sickness and disability benefits. The same fatally flawed BPS model of assessment adopted for the WCA in 2008 to limit access to the Employment and Support Allowance (ESA) is now used by the DWP to limit access to the new Universal Credit, for illness, which is being rolled out across the UK to replace several social security benefits, including the ESA, and is guaranteed to create more preventable harm to many.
In particular, the WCA has been used since October 2008 to restrict access to the Employment and Support Allowance (ESA), and the WCA is also used by the Veterans Agency to restrict increases in military War Pensions for older disabled veterans, despite the fact that a War Pension is not a benefit.
Administered by the DWP, the ESA replaced the former Incapacity Benefit and is the begrudged UK long-term benefit for chronically ill and disabled people who are unfit to work. The ongoing political assault against the chronically ill and disabled community was inspired by the the 2001 ‘Malingering and Illness Deception Conference ’, held in Oxford, where UnumProvident Insurance joined forces with various visiting foreign Psychologists; and representatives of the DWP, and concluded that the majority of claimants of long-term sickness benefit should be ‘motivated’ to find employment.
‘What linked many of them together, including Aylward, was their association
with the giant US income protection company UnumProvident, represented at the
conference by John LoCascio… The cultural meaning of illness would be
redefined; growing numbers of claimants would be declared capable of work and
‘motivated’ into jobs. “Two factors threatened future profits
however. The first was falling interest rates, and the second was the growth
in new kinds of ‘subjective illnesses’, for which diagnostic tests
were disputable. The old industrial injuries were giving way to illnesses with
no clear biological markers – Myalgic Encephalomyelitis (ME) or Chronic
Fatigue Syndrome (CFS), Fibromyalgia, Chronic Pain, Multiple Sclerosis, Lyme
Disease. In the early 1990s the new kinds of claims began to rise just as interest
rates fell: profits were threatened. Unum’s 1995 ‘Chronic Fatigue
Syndrome Management Plan’ sounded the alarm: ‘Unum stands to lose
millions if we do not move quickly to address this increasing problem’.’
Government and Insurance companies – establishing the BPS model
Science for ME: Where Science and the ME/CFS Community Meet
To meet that goal, the WCA uses a discredited biopsychosocial (BPS) model of
assessment, justified by academic research commissioned by the British government
in 2005, when funded by the government corporate ‘advisers ’ UnumProvident
Insurance. By adopting the fatally flawed Waddell and Aylward BPS assessment
model, the WCA presumes that all ESA claimants are potentially bogus. Influenced
by the American corporate advisers, the WCA is described as a ‘ non-medical
functional assessment ’ and so it totally disregards diagnosis, prognosis
and all medical opinion which is very dangerous and cannot possibly be justified.
It is the abdication of all ethical and moral responsibility for the welfare
and wellbeing of the chronically sick and disabled community, who are financially
dependent upon the State, by permitting the fatally flawed WCA to be conducted
by the unaccountable private sector.
The WCA is the adoption of a replica of the BPS ‘disability denial ’
assessment model, as used by Unum (Provident) Insurance to resist funding income
protection healthcare insurance claims. It was willingly adopted by the DWP
to reduce access to the welfare budget, regardless of the inevitable human consequences.
In 2010 the Cameron coalition government increased the resistance to funding
ESA, whilst demonising claimants of long-term sickness benefit which the tabloid
press happily reported in banner headlines for the next five years. Savage sanctions
were imposed for minor transgressions, which can stop benefit for months resulting
in some chronically ill people starving to death in C21st UK, and others being
admitted to hospital in a coma.
Big Problems:
Government appear so determined to get more PAs, AAs into the system
- by bribing GMC to register them on same database as real Doctors
-by employing more without Leng review confirming safe, and scope
-by conrtinuing ARRS funding of PAs, not Doctors
-blocking GPs training paths in favour of PAs
-ban PAs, AAs- a drag on GPs, a drag on hospital care!
Streeting
-applies no improvements
-delay after delay
-waiting for Musk and Trump inauguration
-waiting for US trade deal to include our NHS
-buyout by Musk, Black Rock
-delay FPR, more medics leave
-understaffing- no plan for more Doctors, Nurses, Midwives, Radiologists, Oncologists
-beds being reduced and reduced
-no admission to triage cubicles for A&E, no assess to discharge cubicles
for discharge plans
-no Care progress
-need Care workers with career progression, NHS rates of pay, training, merit
awards
Alienates NHS and SC workers "the NHS is broken"
-believes in NHS app to persuade patients to travel miles to, say, Frinton General,
go private, go chop shop…
-continues to give NHS funds to private hospital chains-who have little capacity,
cherry pick simple cases, have no Intensive Care Unit, no night staff, steal
NHS teams, destabilise NHS teams
-conrinues to favour PFI, private equity- high extortionate interest rates,
bancrups hospitals...
-continues to decimate NHS dentistry…
Obvious measures:
Recover Di Do’s £37 billion
Tax oil
Tax Google, Amazon,
Ensure all taxes due are collected
Ban overseas tax havens
Ban smoking, lose weight, cut sugar, cut salt
Keep the US out of our NHS
More ambulances, drivers, paramedics, admission cubicles
More A&E staff, beds,
This government have proven beyond doubt that manifesto
pledges, promises, priorities are not worth anything.
Blair said Do anything nasty in the first few months- electorate will have forgotten”
Oh no we won’t…
The report concludes that switching to an SHI system would be costly and disruptive, with no evidence it would deliver benefits. Instead, UK policymakers should recognise the strengths of the UK’s existing model – low administrative costs and low financial barriers to care compared with other countries – and focus on how to secure long-term sustainable funding in the face of growing demand.
Just Treatment
Campaigns
Tackling the NHS crisis
Right to Breathe
Youth mental health
Protect patient data
Past campaigns
UpdatesJoinShopDonate
??Facebook??Twitter/X??Instagram?TikTok??Get in touch??Privacy
Labour & the NHS: new year, same
dangerous mistakes
The new government is bringing urgently needed energy to the NHS crisis, but
the swathe of policy announcements made this week risk repeating pro-privatisation
mistakes of the past with dangerous implications for the future of our public
health service.
As a new year begins, our NHS has once again been plunged into crisis. This
week multiple NHS trusts were forced to declare critical incidents due to “exceptionally
high demands” in emergency departments. One patient had to wait 50 hours
to be admitted to a ward.
These life-threatening delays are all-too-familiar for patients. The Labour
government, who have now been in power for 6 months, have pledged to tackle
waiting lists and the NHS backlog. Yet so far, little meaningful progress has
been made.
Over the last week Labour have come out with a series of further announcements
about their plans to fix the NHS crisis. In this blog we break down what they’re
promising, what it means for patients, and what’s missing…
Social care
First up, Health Secretary Wes Streeting announced that the government is launching
an independent commission to reform social care and create a National Care Service.
Everyone knows that fixing social care is an absolutely essential part of rebuilding
our health service - the dangerous bottle necks we see in hospitals across the
country are so often caused by a lack of beds, which in turn are caused by an
inability to discharge vulnerable patients back into the community due to a
lack of available care.
So major reform to social care is essential - and it’s also urgent. But
here’s the catch. At the same time as announcing this commission, the
government also admitted that any reforms would not come into practice until
at least 2028.
Three years waiting for a proposal on how to solve the social care crisis, followed by however long it takes to agree and implement a plan, followed by another wait for the effects to kick in is far more years than patients, carers, and the NHS can wait. This huge delay will cost lives. What patients and the NHS really need is a plan funded by progressive taxation, implemented in the next 18 months.
Waiting lists, funding & staffing
A few days later, Keir Starmer announced a plan to reduce waiting lists and
tackle hospital backlogs. He said that the new government target is to reach
65% of patients beginning treatment or being given the all clear within 18 weeks
by March 2026.
Specific policies in this plan include:
Expanding the network of community diagnostic centres and surgical hubs, to
enable more treatment outside of hospitals
An upgrade to the NHS app which will allegedly make it easier to exercise patient
choice about where they are treated
More direct referrals for testing and scans
Some of these reforms are welcome, and could make a positive difference to patients. However, as we’ve been saying since day one of the Labour government, reform means nothing without the urgently needed uplifts in the NHS budget after more than a decade of cuts and underfunding. The modest funding increase announced in the Autumn Budget is at best around a quarter of the additional funds the NHS truly needs, according to Health Foundation calculations.
Alongside urgent investment in repairing and increasing hospital capacity, the single most important thing the government could be doing to solve the NHS crisis is investment in tackling the staffing crisis. Yet these plans reflect no policies aimed at improving pay and conditions such that the NHS can retain the people it needs. In fact, it is likely to exacerbate staff shortages as a huge growth in private provision means more staff are set to be poached to work outside the NHS.
Further privatisation
As part of these reforms, Starmer worryingly announced a new deal with the “independent
sector” (code for private companies) which will see more NHS patients
being treated in profit-making clinics. This will mean that the private sector’s
role in cutting NHS waiting lists in England will rise by 20%.
The government is using the crisis in the NHS as an opportunity to dramatically increase the privatisation of our public health service, with one in five non-emergency appointments, tests, and operations set to be performed by private providers. This doubling in the size of privatised NHS care will mean £16bn a year of taxpayer money is diverted from public NHS facilities to fuel corporate profits.
This is an unnecessary, damaging, and ideologically-driven action. This money could be better invested in building up NHS capacity to deliver this care. The private sector will only be able to deliver on it by poaching NHS staff, and it accelerates a vicious cycle that further weakens the NHS and makes it ever more reliant on the private sector. As we’ve said many times before, the private sector is not and never will be the solution!
Tech & accountability
Finally, many people will welcome a far more user friendly and powerful NHS
app - if it can be delivered. But there needs to be clear safeguards to ensure
it doesn’t exacerbate digital exclusion, or act as a barrier to patients
seeing NHS staff face to face if they need to.
Furthermore, the reforms the government has been making in how our health data is used need to be paused to allow for proper consultation on the reality of their implications instead of being rammed through, as we have seen with the Federated Data Platform run by the military spy tech corporation Palantir.
Patients should have a say in how our personal data is used and managed. We want it to be used to benefit health outcomes, not to make money for unaccountable and unethical private corporations!
Amidst plunging polls and favourability, Labour are desperate to convince the British public that they care about the NHS-but the problem is, they continue to repeat the same mistakes of past governments by refusing to meaningfully invest in the NHS and instead diverting public funds into the pockets of private healthcare.
With their major 10 year plan for the NHS set to launch in March, alongside their first Spring Budget, it is vital that Labour correct course by rejecting privatisation and generating new funds for our NHS by taxing corporations and the rich.
Just Treatment will continue to fight for these changes - join us.
Short sighted idiotic policies:
Thatcher allowed local authorities to recoup residents Income Support,
(the residential allowance)
Thatcher & Major sold hundreds of care homes for £1 each (value £2.03
million
to get rid of care homes, move residents into independent, for profit homes
transferring public assets to for profit providers at little or no cost
The policy of shunting care local authorities allowed the NHS to sell
off associated land and buildings
small cottage hospitals, such as Oxted and Limpsfield War Memorial Hospital-tranquil
oasis, lots of land developers had their eye on… services simply disappeared
Trusts were urged, told to sell of “surplus” land, or charged
heavily,
They now are short of land for rebuilds, extensions, designated free staff parking…
All extremely short-sighted policy
Politician have no long term strategy-they will be long gone in five year’s
time!
all under the lie of “care in the community”-more workload for frazzled GPs…
Operose practice
stuffed with PAs
https://www.bbc.co.uk/news/health-61759641

Latest wheezes rather than invest…
Ambulance “listen and treat”
call handlers with a script try to avoid an ambulance call-out by treating by
telephone
We need a prudent surplus of ambulances, paramedics, fast offload, not run-on-the-limit
Treat A & E patients at home
very risky-poor results
time-consuming
depends on broadband, hardware and software, patient training, frontline training
nobody chooses to go to A & E voluntarily-six hours standing…
Build cubicles to receive and triage-fast unload of ambulances
Build assess to discharge cubicles-empty real beds into cubicles-staffed
NHS and Social Care plans based on fantasy...
Streeting is delaying everything, cutting targets, and hopes that AI, NHS apps, new tecnology will bale the NHS out.
The NHS needs better, reliable basic IT in GP practices and hospitals
but MORE FRONTLINE STAFF: doctors, nurses, midwives, beds, operations...
No point in more scans and cancer diagnosis if treatment is delayed...